The goals for treating persons with chronic hepatitis C virus (HCV) are threefold: (1) eradicate HCV, (2) improve HCV-related health outcomes and survival, and (3) reduce transmission of HCV to others. With the current armamentarium of highly effective and safe direct-acting antiviral (DAA) medications, cure of chronic HCV is expected in more than 95% of persons receiving HCV treatment, regardless of HCV genotype, baseline HCV RNA levels, race, HIV status, or severity of hepatic fibrosis.[1,2] The health outcome benefits following successful treatment of persons with chronic HCV infection are multiple and include reduced prevalence of hepatic fibrosis, lower risk of developing hepatic failure, decreased occurrence of hepatocellular carcinoma (HCC), improved survival, and amelioration of some extrahepatic HCV-related manifestations.[3,4,5,6] With widespread treatment of HCV, the number of persons capable of transmitting HCV would decline dramatically, which could have a major impact on HCV incidence and the overall HCV epidemic.
- Module 4 Overview
Evaluation and Preparation for Hepatitis C Treatment - Lesson 1
Goals and Benefits with HCV TreatmentLesson 1. Goals and Benefits with HCV Treatment
PDF ShareLast Updated: April 2nd, 2024Authors:H. Nina Kim, MD, MSc,H. Nina Kim, MD, MSc
Associate Editor
Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneMaria A. Corcorran, MD, MPHMaria A. Corcorran, MD, MPH
Associate Editor
Assistant Professor
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneReviewer:David H. Spach, MDDavid H. Spach, MD
Editor-in-Chief
Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneLearning Objective Performance Indicators
- Cite the goals and rationale for HCV therapy in persons with chronic HCV
- Discuss durability of sustained virologic response when achieved with direct-acting antiviral therapy
- List several long-term benefits of HCV treatment on clinical outcomes in persons with chronic HCV
- Describe the impact of HCV treatment on survival
- Summarize the population-level benefit of HCV treatment
Table of ContentsBackground
Virologic Cure and Sustained Virologic Response
HCV Eradication and Sustained Virologic Response (SVR)
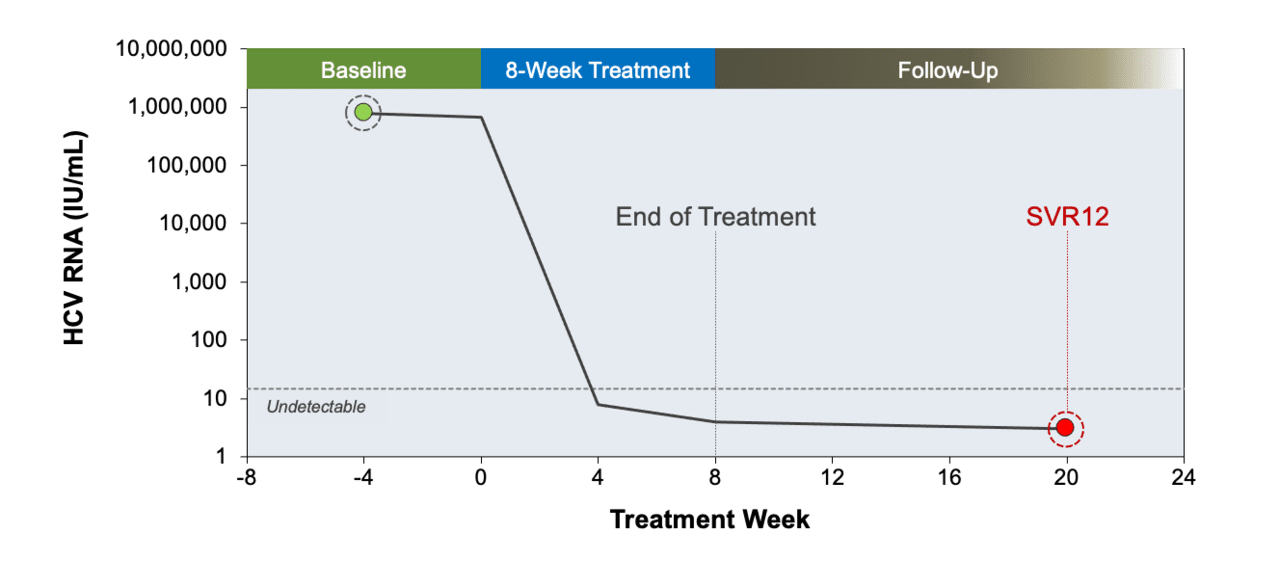
The gold standard for determining cure of HCV is the demonstration of sustained undetectable HCV RNA levels after treatment.[7] A sustained virologic response (SVR) is an undetectable HCV RNA level using a sensitive assay (typically with a lower limit of 25 IU/mL) at least 12 weeks after completing HCV therapy (Figure 1).[8] In the current era, most expert guidelines recommend measuring an HCV RNA level 12 weeks after therapy to evaluate for SVR; individuals with an undetectable HCV RNA level at 12-weeks posttreatment, also known as an SVR12, are considered to have achieved a virologic cure.[7] Among persons who achieve an SVR12 with direct-acting antiviral (DAA) HCV therapy, greater than 99% go on to achieve a durable response and ongoing absence of detectable viremia.[9,10] Achieving SVR4, which represents undetectable HCV RNA 4 weeks after treatment completion, has high concordance (on the order of 98-99%) with SVR12 and could be considered as an alternative endpoint for final assessment of viral clearance, but SVR12 remains the consensus outcome.[11,12]
Durability of SVR
Long-term follow-up of persons who achieve an SVR12 has shown that nearly 100% remain HCV RNA-negative years after therapy, unless they are reinfected with HCV.[13,14,15] Several large studies have shown a negligible relapse rate, between 0 and 1% at 4 or 5 years, with either interferon-based or DAA-based therapy.[16,17,18] Thus, an undetectable HCV RNA 12 or 24 weeks after antiviral therapy can be considered a virologic cure. It is important to note that persons cured of HCV can become reinfected with HCV.[17,19]
Impact of HCV Treatment on Clinical Outcomes
Impact of HCV Treatment on Hepatic Fibrosis
Individuals who achieve an SVR are more likely to have an improvement in liver inflammation and fibrosis than those who do not achieve an SVR.[20,21,22,23] The following studies highlight data related to the impact of HCV eradication on hepatic fibrosis. Of note, a number of studies have examined posttreatment transient elastography which can overestimate the regression in fibrosis, probably because of reduced hepatic inflammation and congestion.
- In a pooled analysis of adults who had paired liver biopsies before and 1 month to 6 years after treatment with interferon-based therapies, individuals who achieved an SVR were twice as likely to have lower necroinflammatory scores after treatment, compared to those with virologic relapse (67% versus 32%), and some patients with an SVR had complete regression of liver fibrosis.[23]
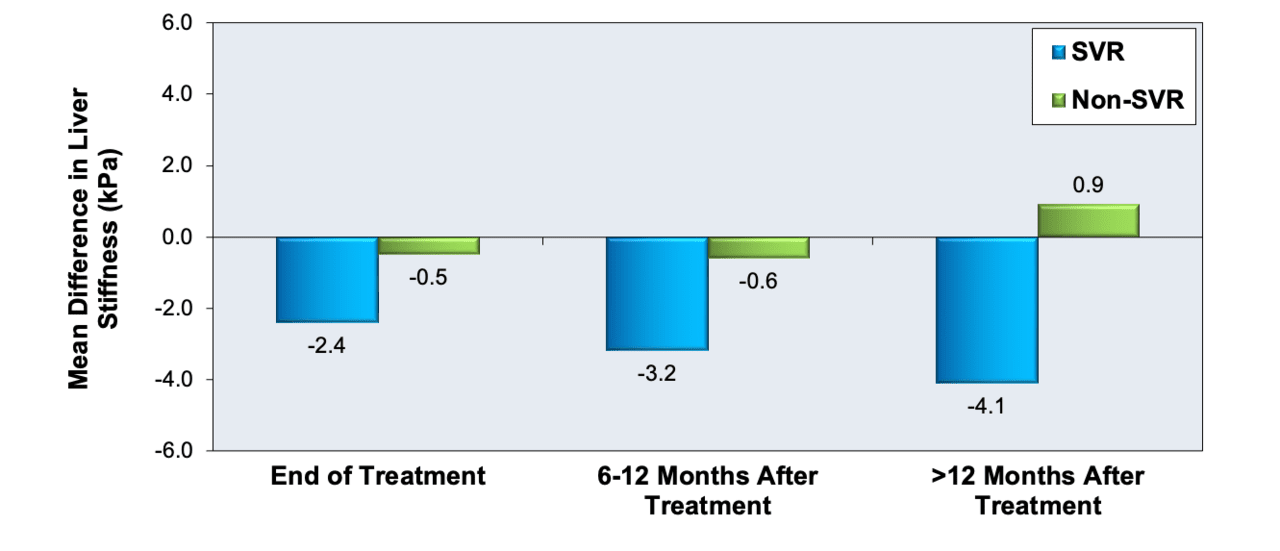
- In a meta-analysis, investigators evaluated the impact of HCV treatment on liver stiffness, as measured by vibration-controlled transient elastography.[20] Individuals who achieved an SVR12 had a significantly greater decrease in liver stiffness at the end of treatment and after treatment than patients who failed to achieve an SVR12 (Figure 2).[20] In addition, the decline in liver stiffness among those who achieved an SVR12 was greater with DAA treatment than with interferon-based therapy (decrease of 5.1 kPa versus decrease of 2.8 kPa).[20]
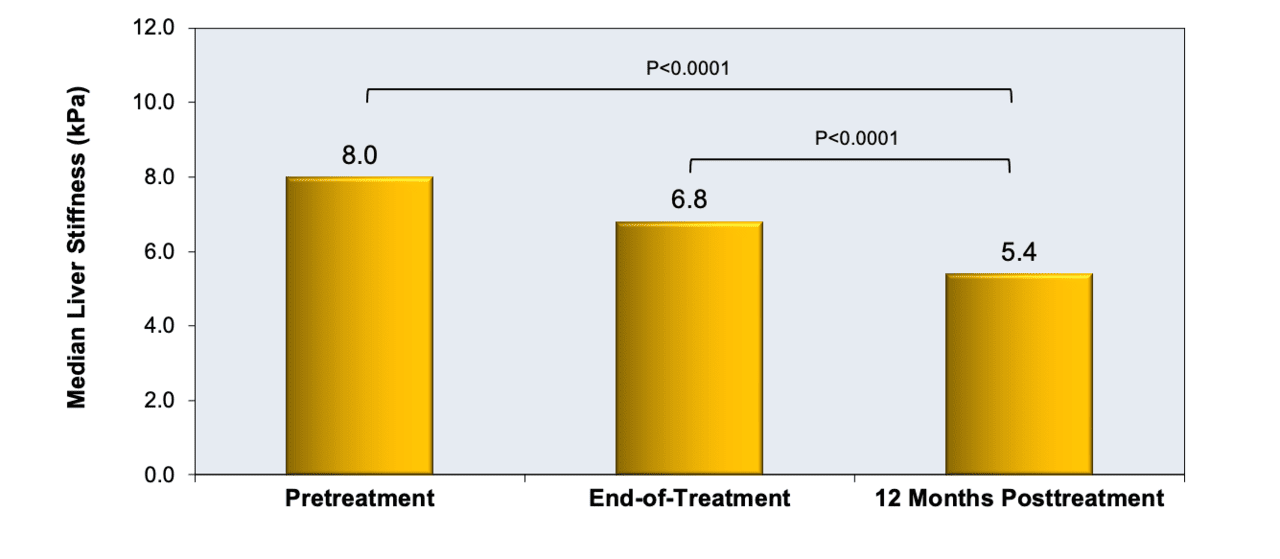
- In a study, investigators performed liver stiffness measurements in 70 patients treated with DAA therapy, among whom 95.7% achieved an SVR.[21] Treatment of HCV with DAA therapy resulted in a significant decrease in liver stiffness at the end of treatment and at 12 months posttreatment when compared with baseline measurements (Figure 3).[21]
- In a multi-center, prospective cohort study that enrolled 71 Danish adults with advanced fibrosis, investigators found that liver stiffness decreased by an average of 20% at the end of sofosbuvir-based direct-acting antiviral therapy, and by an additional 15% 1 year after treatment, a finding that was suggestive of fibrosis regression.[24]
Impact of HCV Treatment on Hepatocellular Carcinoma
- Multiple studies have shown a reduction in the risk of HCC occurrence after achievement of SVR with HCV therapy; in these studies, control groups consisted of persons with HCV who were treated but did not achieve an SVR.[4,25,26,27] Several of the more recent studies exclusively involved persons treated with DAA therapy.[26,28,29]
- Although HCV eradication with HCV therapy can reduce the long-term risk of HCC, the risk of developing HCC remains substantial for persons who, prior to treatment, had advanced fibrosis or cirrhosis.[29] Accordingly, individuals who met HCC surveillance criteria prior to HCV treatment should continue to receive HCC surveillance every 6 months, even after achieving an SVR with HCV treatment.[8,29,30]
- Among persons with a history of successfully treated HCC, there are conflicting data regarding the impact of DAA therapy on the risk of HCC recurrence, with most studies reporting no difference in the risk of recurrent HCC among DAA-treated and untreated persons. As such, DAA-treated individuals with a history of HCC require close ongoing HCC surveillance.[30,31,32,33,34]
Impact of HCV Treatment on Extrahepatic Manifestations
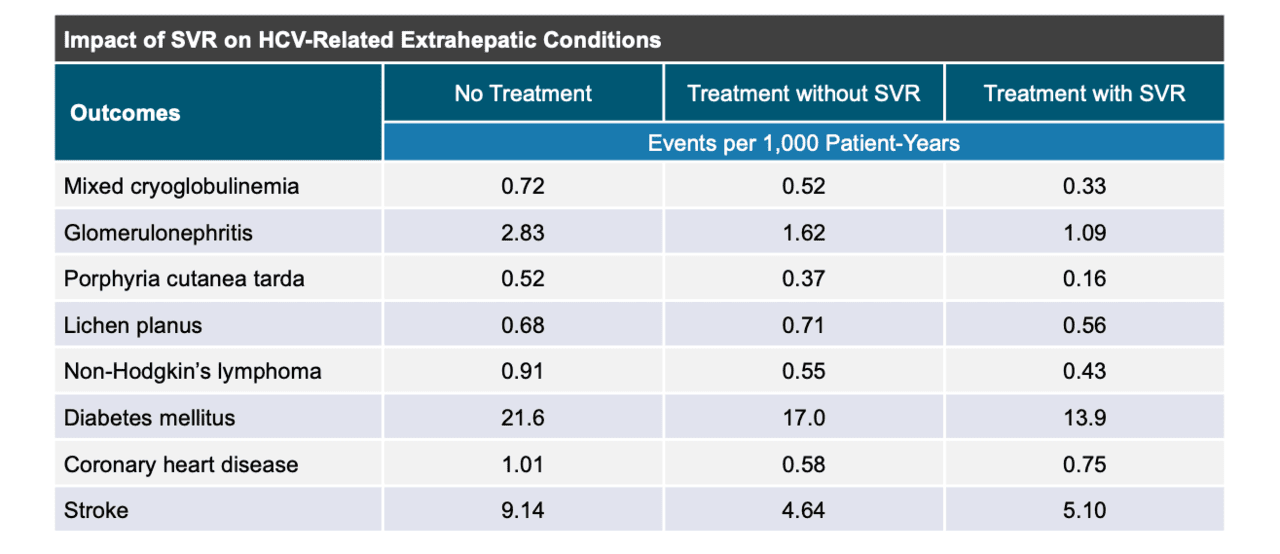
Infection with HCV can cause a myriad of extrahepatic complications, including cryoglobulinemia, membranoproliferative glomerulonephritis, dermatologic disorders, insulin resistance and diabetes mellitus, and B-cell non-Hodgkin's lymphoma.[35,36,37] For a more detailed discussion of this topic, see the lesson Extrahepatic Conditions Related to HCV Infection. There is evidence that the risk of HCV-related extrahepatic manifestations is lower after eradication of HCV with DAA therapy.[38,39] Most notably, in a retrospective cohort study that involved 160,875 United States veterans with chronic HCV, patients who achieved an SVR12 with interferon-based therapy had substantial reductions in HCV-related extrahepatic manifestations when compared with individuals who did not achieve an SVR with HCV treatment or were not treated at all (Figure 4).[40] In some patients, successful treatment of HCV is associated with improvement or remission of these underlying conditions.[41,42] In addition, achieving an SVR has been shown to reduce the chance of impaired fasting glucose and diabetes development by 50%, an effect that is independent of other established risk factors for diabetes, such as age and body mass index. A recent meta-analysis of 48 studies showed that an SVR reduced extrahepatic mortality by 56%, improved response to malignant B-cell lymphoproliferative therapy, and vastly improved the chances of a complete resolution of cryoglobulinemic vasculitis.[3]
Impact of HCV Treatment on Quality of Life
A subset of patients with chronic HCV can experience symptoms of functional impairment that include fatigue or reduced mental stamina.[36] Studies on the impact of SVR with HCV therapy have consistently demonstrated significant improvements in health-related quality of life. Patients who achieve SVR often report reduced fatigue, improved physical functioning, and enhanced mental health compared to those who do not achieve SVR or remain untreated.[43,44,45,46] This improvement in patient-reported outcomes has been observed in advanced disease as well as in people with HCV and HIV coinfection. Further, achieving an SVR with HCV treatment can lead to improvements in work productivity. These results underscore the anticipated economic benefits of successful HCV treatment, with decreased work-related limitations and increased workforce participation. Most of the data on the relationship between HCV treatment and quality of life have been generated from clinical trial participants. Published reports of patient experiences with SVR across a broad sociodemographic and community spectrum remain limited at this time.
Impact of HCV Treatment on Survival
In persons with chronic HCV infection, treatment with achievement of SVR12 or SVR24 has been shown to markedly reduce the risk of death, including liver-related and non-liver-related deaths.[6,16,47,48] Studies have shown survival benefit in persons with chronic HCV (with or without advanced liver disease) who achieve SVR with DAA therapy.[49,50] The following summarizes key data related to the impact of DAA therapy on survival after achieving an SVR.
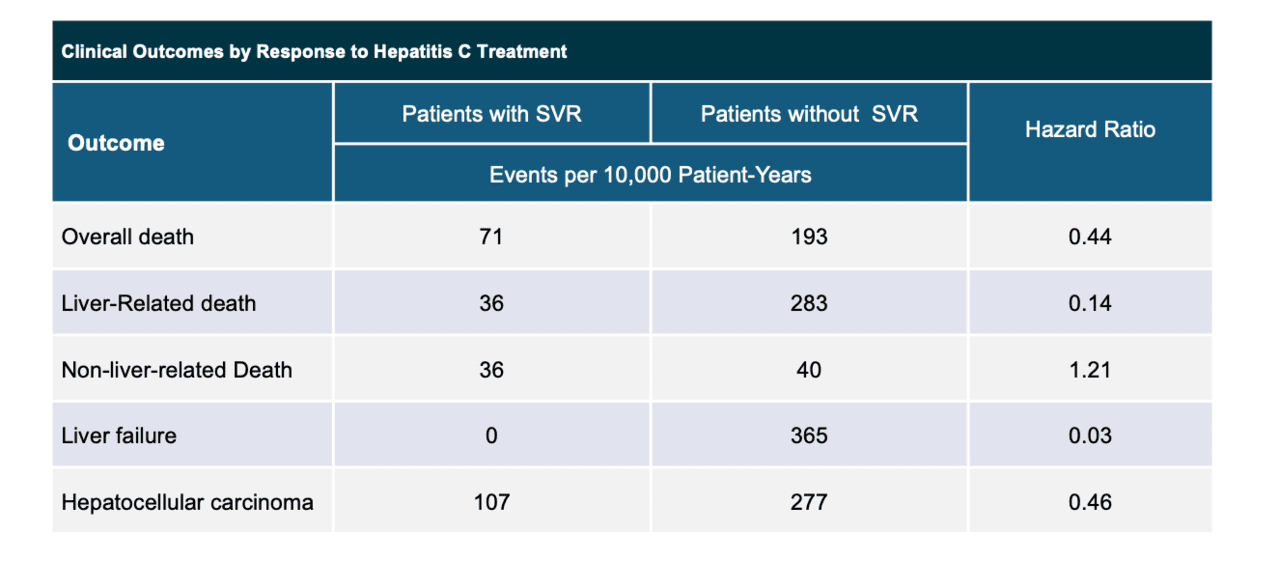
- In a retrospective cohort study, investigators examined the impact of HCV treatment during the years 1990 and 2003 in 5 hepatology units in Europe and Canada.[51] Individuals with advanced fibrosis who underwent antiviral therapy and achieved an SVR had reduced overall mortality, liver-related death, liver failure, and hepatocellular carcinoma compared with those who did not achieve an SVR (Figure 5).[51]
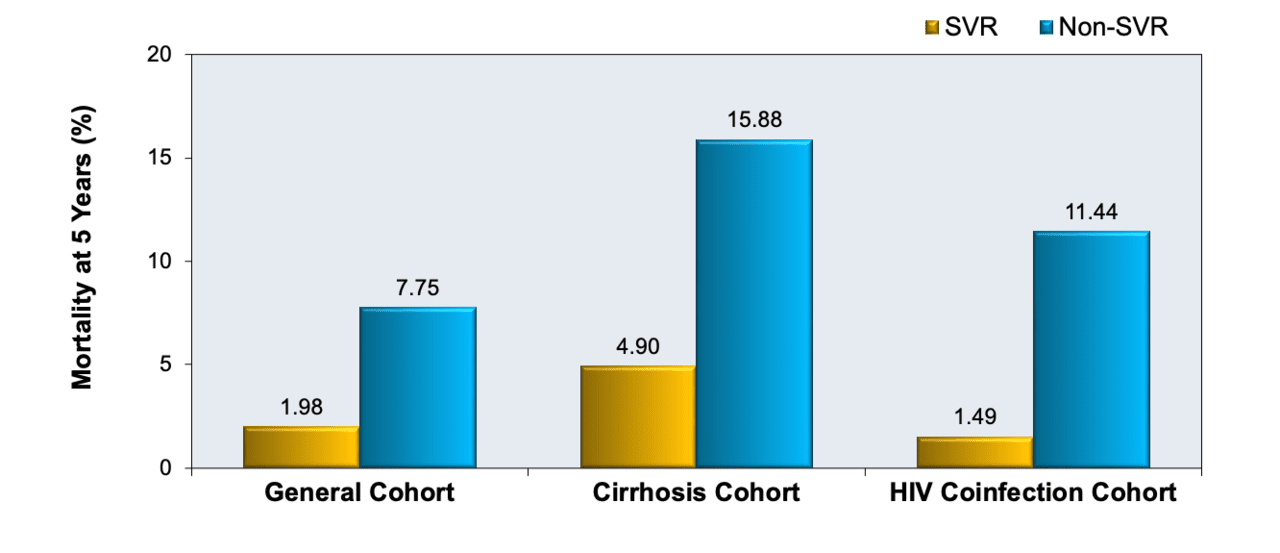
- In a meta-analysis of 35 studies that included 33,360 persons with chronic HCV infection, investigators showed a clear benefit in 5-year overall survival in persons who achieved an SVR with treatment when compared with those who had not achieved an SVR.[52] All the studies analyzed involved interferon-based therapies, and some included individuals with cirrhosis or persons with HIV coinfection (Figure 6).[52]
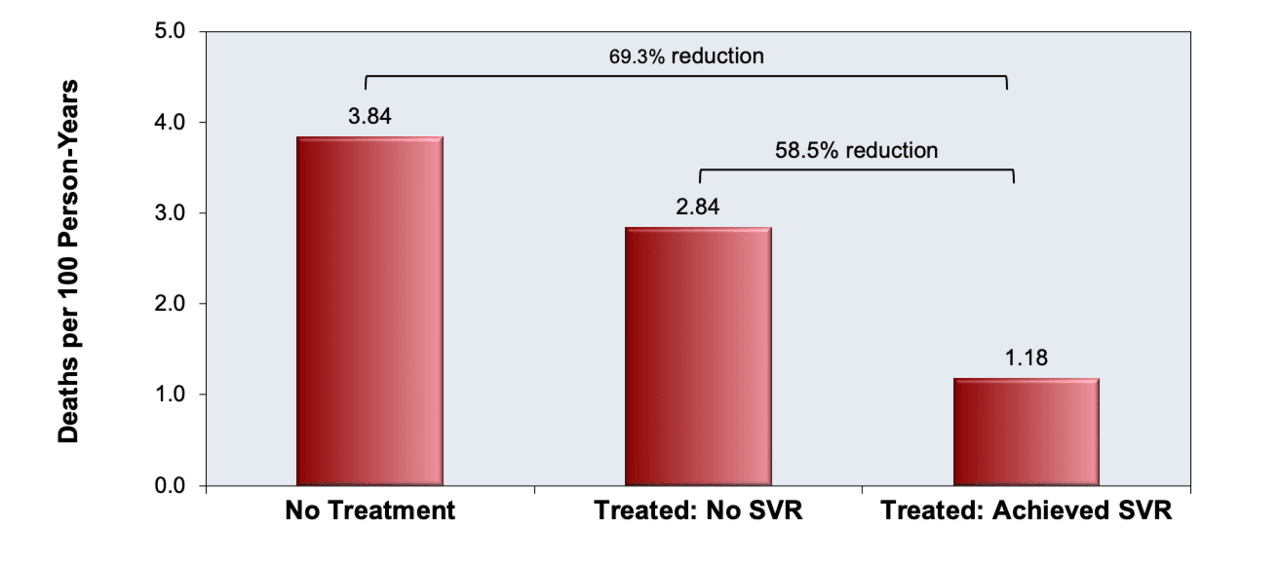
- In an observational cohort analysis of 103,346 persons with chronic HCV (genotype 1, 2, or 3) in the Veterans Affairs Hepatitis C Clinical Case Registry, investigators examined the impact of achieving SVR with DAA treatment on mortality.[49] Among the 40,664 persons treated with a DAA regimen, 39,374 (96.8%) achieved an SVR. The mortality rate in persons who achieved an SVR was significantly lower than in those who did not achieve an SVR with treatment, after adjusting for baseline demographics, clinical characteristics, and comorbidity (Figure 7).[49] The reduction in mortality was 69.3% among those who achieved an SVR compared to persons who did not receive HCV treatment.[49]
- Two separate cohort studies of persons with HCV and successfully treated HCC have found a significantly lower overall risk of death among persons who receive DAA therapy when compared to those who do not, suggesting that selected patients with a history of HCC should receive HCV DAA treatment due to multiple treatment-related benefits, including overall improved survival.[53,54]
- A number of studies evaluating contemporary trends have suggested an early signal of benefit since the introduction of DAA therapy with decreased hospitalization, longer survival, and reduced liver transplantation rates in patients with advanced HCV liver disease.[55,56,57]
Population-Level Benefits of HCV Elimination
In addition to the benefit that HCV treatment provides to the individual, HCV treatment has health and economic benefits at the population level. Modeling studies have shown that treatment of HCV in persons at high risk of transmitting HCV to others, particularly people who inject drugs (PWID), can lead to substantial reductions in HCV incidence and prevalence.[58,59,60,61] This strategy, which is known as treatment as prevention, has also been shown to facilitate real-world HCV microelimination efforts among key populations, including incarcerated individuals, and persons with HIV.[62,63,64,65,66] In addition to preventing person-to-person transmission of HCV and facilitating population-level microelimination, HCV treatment has also been shown to be cost-effective at a population level, with substantial cost savings incurred by avoiding the costly long-term outcomes of HCV, including cirrhosis, end-stage liver disease, and hepatocellular carcinoma.[67,68,69,70] In one recent United States-based costing analysis, authors estimated that between 2013 and 2022, treatment of HCV with DAAs provided a $15 million net economic benefit to Medicaid, with $43 million in cumulative net savings to Medicaid estimated by the end of 2026.[71]
Summary Points
- There are multiple goals with HCV antiviral therapy, including (1) eradicate HCV, (2) improve HCV-related health outcomes and survival in all populations, and (3) reduce transmission of HCV to others.
- A sustained virologic response is defined as an undetectable HCV RNA level 12 weeks after stopping antivirals; this is referred to as the SVR12, and the SVR12 has a high correlation with SVR24. An SVR is durable and indicates HCV cure.
- Achieving an SVR following HCV treatment results in improvement of hepatic fibrosis, decreased development of HCC, improvement in survival, and reduction in extrahepatic manifestations associated with chronic HCV.
- In the DAA treatment era, HCV genotype has a reduced role in predicting treatment response given the availability of a variety of DAA combinations with high efficacy across genotypes.
- Older patients, including persons 70 years of age and older, have comparable responses to DAA therapy when compared with younger patients.
- With newer DAA therapies, individuals with more advanced fibrosis and compensated cirrhosis typically have HCV treatment SVR rates greater than 95% with 12-week treatment regimens. Persons with decompensated cirrhosis are more difficult to treat and often have reduced response rates.
Citations
- 1.Asselah T, Marcellin P, Schinazi RF. Treatment of hepatitis C virus infection with direct-acting antiviral agents: 100% cure? Liver Int. 2018;38 Suppl 1:7-13.[PubMed Abstract] -
- 2.Marcellin F, Roux P, Protopopescu C, Duracinsky M, Spire B, Carrieri MP. Patient-reported outcomes with direct-acting antivirals for the treatment of chronic hepatitis C: current knowledge and outstanding issues. Expert Rev Gastroenterol Hepatol. 2017;11:259-268.[PubMed Abstract] -
- 3.Cacoub P, Desbois AC, Comarmond C, Saadoun D. Impact of sustained virological response on the extrahepatic manifestations of chronic hepatitis C: a meta-analysis. Gut. 2018;67:2025-34.[PubMed Abstract] -
- 4.Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158:329-37.[PubMed Abstract] -
- 5.Tada T, Kumada T, Toyoda H, et al. Viral eradication reduces all-cause mortality, including non-liver-related disease, in patients with progressive hepatitis C virus-related fibrosis. J Gastroenterol Hepatol. 2017;32:687-694.[PubMed Abstract] -
- 6.van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308:2584-93.[PubMed Abstract] -
- 7.AASLD-IDSA. HCV Guidance: Recommendations for testing, management, and treating hepatitis C. When and in whom to initiate HCV therapy.
- 8.AASLD-IDSA. HCV Guidance: Recommendations for testing, management, and treating hepatitis C. Monitoring patients who are starting HCV treatment, are on treatment, or have completed therapy.
- 9.Burgess SV, Hussaini T, Yoshida EM. Concordance of sustained virologic response at weeks 4, 12 and 24 post-treatment of hepatitis c in the era of new oral direct-acting antivirals: A concise review. Ann Hepatol. 2016;15:154-9.[PubMed Abstract] -
- 10.Martinot-Peignoux M, Stern C, Maylin S, et al. Twelve weeks posttreatment follow-up is as relevant as 24 weeks to determine the sustained virologic response in patients with hepatitis C virus receiving pegylated interferon and ribavirin. Hepatology. 2010;51:1122-6.[PubMed Abstract] -
- 11.Gane E, de Ledinghen V, Dylla DE, et al. Positive predictive value of sustained virologic response 4 weeks posttreatment for achieving sustained virologic response 12 weeks posttreatment in patients receiving glecaprevir/pibrentasvir in Phase 2 and 3 clinical trials. J Viral Hepat. 2021;28:1635-42.[PubMed Abstract] -
- 12.Yoshida EM, Sulkowski MS, Gane EJ, et al. Concordance of sustained virological response 4, 12, and 24 weeks post-treatment with sofosbuvir-containing regimens for hepatitis C virus. Hepatology. 2015;61:41-5.[PubMed Abstract] -
- 13.George SL, Bacon BR, Brunt EM, Mihindukulasuriya KL, Hoffmann J, Di Bisceglie AM. Clinical, virologic, histologic, and biochemical outcomes after successful HCV therapy: a 5-year follow-up of 150 patients. Hepatology. 2009;49:729-38.[PubMed Abstract] -
- 14.Maylin S, Martinot-Peignoux M, Moucari R, et al. Eradication of hepatitis C virus in patients successfully treated for chronic hepatitis C. Gastroenterology. 2008;135:821-9.[PubMed Abstract] -
- 15.Morisco F, Granata R, Stroffolini T, et al. Sustained virological response: a milestone in the treatment of chronic hepatitis C. World J Gastroenterol. 2013;19:2793-8.[PubMed Abstract] -
- 16.Pearlman BL, Traub N. Sustained virologic response to antiviral therapy for chronic hepatitis C virus infection: a cure and so much more. Clin Infect Dis. 2011;52:889-900.[PubMed Abstract] -
- 17.Simmons B, Saleem J, Hill A, Riley RD, Cooke GS. Risk of Late Relapse or Reinfection With Hepatitis C Virus After Achieving a Sustained Virological Response: A Systematic Review and Meta-analysis. Clin Infect Dis. 2016;62:683-694.[PubMed Abstract] -
- 18.Lin CP, Liang PC, Huang CI, et al. Concordance of SVR12, SVR24 and SVR durability in Taiwanese chronic hepatitis C patients with direct-acting antivirals. PLoS One. 2021;16:e0245479.[PubMed Abstract] -
- 19.Page K, Hahn JA, Evans J, et al. Acute hepatitis C virus infection in young adult injection drug users: a prospective study of incident infection, resolution, and reinfection. J Infect Dis. 2009;200:1216-26.[PubMed Abstract] -
- 20.Singh S, Facciorusso A, Loomba R, Falck-Ytter YT. Magnitude and Kinetics of Decrease in Liver Stiffness After Antiviral Therapy in Patients With Chronic Hepatitis C: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16:27-38.e4.[PubMed Abstract] -
- 21.Chan J, Gogela N, Zheng H, et al. Direct-Acting Antiviral Therapy for Chronic HCV Infection Results in Liver Stiffness Regression Over 12 Months Post-treatment. Dig Dis Sci. 2018;63:486-492.[PubMed Abstract] -
- 22.Poynard T, McHutchison J, Manns M, et al. Impact of pegylated interferon alfa-2b and ribavirin on liver fibrosis in patients with chronic hepatitis C. Gastroenterology. 2002;122:1303-13.[PubMed Abstract] -
- 23.Pockros PJ, Hamzeh FM, Martin P, et al. Histologic outcomes in hepatitis C-infected patients with varying degrees of virologic response to interferon-based treatments. Hepatology. 2010;52:1193-200.[PubMed Abstract] -
- 24.Laursen TL, Siggaard CB, Kazankov K, et al. Time-dependent improvement of liver inflammation, fibrosis and metabolic liver function after successful direct-acting antiviral therapy of chronic hepatitis C. J Viral Hepat. 2020;27:28-35.[PubMed Abstract] -
- 25.Ioannou GN, Green PK, Berry K. HCV eradication induced by direct-acting antiviral agents reduces the risk of hepatocellular carcinoma. J Hepatol. 2017. pii: S0168-8278(17)32273-0.[PubMed Abstract] -
- 26.Calvaruso V, Cabibbo G, Cacciola I, et al. Incidence of Hepatocellular Carcinoma in Patients With HCV-Associated Cirrhosis Treated With Direct-Acting Antiviral Agents. Gastroenterology. 2018;155:411-21.e4.[PubMed Abstract] -
- 27.Nahon P, Bourcier V, Layese R, et al. Eradication of Hepatitis C Virus Infection in Patients With Cirrhosis Reduces Risk of Liver and Non-Liver Complications. Gastroenterology. 2017;152:142-156.e2.[PubMed Abstract] -
- 28.Konjeti VR, John BV. Interaction Between Hepatocellular Carcinoma and Hepatitis C Eradication With Direct-acting Antiviral Therapy. Curr Treat Options Gastroenterol. 2018;16:203-214.[PubMed Abstract] -
- 29.Kanwal F, Kramer J, Asch SM, Chayanupatkul M, Cao Y, El-Serag HB. Risk of Hepatocellular Cancer in HCV Patients Treated With Direct-Acting Antiviral Agents. Gastroenterology. 2017;153:996-1005.e1.[PubMed Abstract] -
- 30.Singal AG, Lim JK, Kanwal F. AGA Clinical Practice Update on Interaction Between Oral Direct-Acting Antivirals for Chronic Hepatitis C Infection and Hepatocellular Carcinoma: Expert Review. Gastroenterology. 2019;156:2149-57.[PubMed Abstract] -
- 31.ANRS collaborative study group on hepatocellular carcinoma (ANRS CO22 HEPATHER, CO12 CirVir and CO23 CUPILT cohorts). . Lack of evidence of an effect of direct-acting antivirals on the recurrence of hepatocellular carcinoma: Data from three ANRS cohorts. J Hepatol. 2016;65:734-40.[PubMed Abstract] -
- 32.Cabibbo G, Petta S, Calvaruso V, et al. Is early recurrence of hepatocellular carcinoma in HCV cirrhotic patients affected by treatment with direct-acting antivirals? A prospective multicentre study. Aliment Pharmacol Ther. 2017;46:688-695.[PubMed Abstract] -
- 33.Saraiya N, Yopp AC, Rich NE, Odewole M, Parikh ND, Singal AG. Systematic review with meta-analysis: recurrence of hepatocellular carcinoma following direct-acting antiviral therapy. Aliment Pharmacol Ther. 2018;48:127-37.[PubMed Abstract] -
- 34.Singal AG, Rich NE, Mehta N, et al. Direct-Acting Antiviral Therapy Not Associated With Recurrence of Hepatocellular Carcinoma in a Multicenter North American Cohort Study. Gastroenterology. 2019;156:1683-92.e1.[PubMed Abstract] -
- 35.El-Serag HB, Hampel H, Yeh C, Rabeneck L. Extrahepatic manifestations of hepatitis C among United States male veterans. Hepatology. 2002;36:1439-45.[PubMed Abstract] -
- 36.Jacobson IM, Cacoub P, Dal Maso L, Harrison SA, Younossi ZM. Manifestations of chronic hepatitis C virus infection beyond the liver. Clin Gastroenterol Hepatol. 2010;8:1017-29.[PubMed Abstract] -
- 37.Tang L, Marcell L, Kottilil S. Systemic manifestations of hepatitis C infection. Infect Agent Cancer. 2016;11:29.[PubMed Abstract] -
- 38.Ioannou GN, Feld JJ. What Are the Benefits of a Sustained Virologic Response to Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection? Gastroenterology. 2019;156:446-460.e2.[PubMed Abstract] -
- 39.Li J, Gordon SC, Zhou Y, et al. Sex Differences in Extrahepatic Outcomes After Antiviral Treatment for Hepatitis C. Am J Gastroenterol. 2021;116:576-83.[PubMed Abstract] -
- 40.Mahale P, Engels EA, Li R, et al. The effect of sustained virological response on the risk of extrahepatic manifestations of hepatitis C virus infection. Gut. 2018;67:553-561.[PubMed Abstract] -
- 41.Arase Y, Suzuki F, Suzuki Y, et al. Sustained virological response reduces incidence of onset of type 2 diabetes in chronic hepatitis C. Hepatology. 2009;49:739-44.[PubMed Abstract] -
- 42.Conjeevaram HS, Wahed AS, Afdhal N, Howell CD, Everhart JE, Hoofnagle JH. Changes in insulin sensitivity and body weight during and after peginterferon and ribavirin therapy for hepatitis C. Gastroenterology. 2010;140:469-77.[PubMed Abstract] -
- 43.Younossi ZM, Stepanova M, Afdhal N, et al. Improvement of health-related quality of life and work productivity in chronic hepatitis C patients with early and advanced fibrosis treated with ledipasvir and sofosbuvir. J Hepatol. 2015;63:337-45.[PubMed Abstract] -
- 44.Younossi ZM, Stepanova M, Feld J, et al. Sofosbuvir/velpatasvir improves patient-reported outcomes in HCV patients: Results from ASTRAL-1 placebo-controlled trial. J Hepatol. 2016;65:33-9.[PubMed Abstract] -
- 45.Younossi ZM, Stepanova M, Jacobson IM, et al. Sofosbuvir and velpatasvir with or without voxilaprevir in direct-acting antiviral-naïve chronic hepatitis C: patient-reported outcomes from POLARIS 2 and 3. Aliment Pharmacol Ther. 2018;47:259-67.[PubMed Abstract] -
- 46.Younossi ZM, Stepanova M, Sulkowski M, Wyles D, Kottilil S, Hunt S. Patient-reported outcomes in patients co-infected with hepatitis C virus and human immunodeficiency virus treated with sofosbuvir and velpatasvir: The ASTRAL-5 study. Liver Int. 2017;37:1796-1804.[PubMed Abstract] -
- 47.Backus LI, Boothroyd DB, Phillips BR, Belperio P, Halloran J, Mole LA. A sustained virologic response reduces risk of all-cause mortality in patients with hepatitis C. Clin Gastroenterol Hepatol. 2011;9:509-516.e1.[PubMed Abstract] -
- 48.Berenguer J, Rodríguez E, Miralles P, et al. Sustained virological response to interferon plus ribavirin reduces non-liver-related mortality in patients coinfected with HIV and Hepatitis C virus. Clin Infect Dis. 2012;55:728-36.[PubMed Abstract] -
- 49.Backus LI, Belperio PS, Shahoumian TA, Mole LA. Direct-acting antiviral sustained virologic response: Impact on mortality in patients without advanced liver disease. Hepatology. 2018;68:827-38.[PubMed Abstract] -
- 50.Backus LI, Belperio PS, Shahoumian TA, Mole LA. Impact of Sustained Virologic Response with Direct-Acting Antiviral Treatment on Mortality in Patients with Advanced Liver Disease. Hepatology. 2019;69:487-97.[PubMed Abstract] -
- 51.Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med. 2007;147:677-84.[PubMed Abstract] -
- 52.Simmons B, Saleem J, Heath K, Cooke GS, Hill A. Long-Term Treatment Outcomes of Patients Infected With Hepatitis C Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response. Clin Infect Dis. 2015;61:730-40.[PubMed Abstract] -
- 53.Cabibbo G, Celsa C, Calvaruso V, et al. Direct-acting antivirals after successful treatment of early hepatocellular carcinoma improve survival in HCV-cirrhotic patients. J Hepatol. 2019;71:265-73.[PubMed Abstract] -
- 54.Singal AG, Rich NE, Mehta N, et al. Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection Is Associated With Increased Survival in Patients With a History of Hepatocellular Carcinoma. Gastroenterology. 2019;157:1253-63.e2.[PubMed Abstract] -
- 55.Kim D, Perumpail BJ, Alshuwaykh O, Dennis BB, Cholankeril G, Ahmed A. Changing trends in aetiology-based hospitalizations with end-stage liver disease in the United States from 2016 to 2019. Liver Int. 2022;42:2390-5.[PubMed Abstract] -
- 56.Arora SS, Axley P, Ahmed Z, et al. Decreasing frequency and improved outcomes of hepatitis C-related liver transplantation in the era of direct-acting antivirals - a retrospective cohort study. Transpl Int. 2019;32:854-64.[PubMed Abstract] -
- 57.Kim D, Li AA, Perumpail BJ, et al. Changing Trends in Etiology-Based and Ethnicity-Based Annual Mortality Rates of Cirrhosis and Hepatocellular Carcinoma in the United States. Hepatology. 2019;69:1064-74.[PubMed Abstract] -
- 58.Fraser H, Martin NK, Brummer-Korvenkontio H, et al. Model projections on the impact of HCV treatment in the prevention of HCV transmission among people who inject drugs in Europe. J Hepatol. 2018;68:402-11.[PubMed Abstract] -
- 59.Martin NK, Vickerman P, Grebely J, et al. Hepatitis C virus treatment for prevention among people who inject drugs: Modeling treatment scale-up in the age of direct-acting antivirals. Hepatology. 2013;58:1598-609.[PubMed Abstract] -
- 60.Zelenev A, Li J, Mazhnaya A, Basu S, Altice FL. Hepatitis C virus treatment as prevention in an extended network of people who inject drugs in the USA: a modelling study. Lancet Infect Dis. 2018;18:215-24.[PubMed Abstract] -
- 61.Zelenev A, Li J, Shea P, Hecht R, Altice FL. Modeling Combination Hepatitis C Virus Treatment and Prevention Strategies in a Network of People Who Inject Drugs in the United States. Clin Infect Dis. 2021;72:755-63.[PubMed Abstract] -
- 62.Dhiman RK, Grover GS, Premkumar M, et al. Outcomes of Real-World Integrated HCV Microelimination for People Who Inject Drugs: An expansion of the Punjab Model. EClinicalMedicine. 2021;41:101148.[PubMed Abstract] -
- 63.Hajarizadeh B, Grebely J, Byrne M, et al. Evaluation of hepatitis C treatment-as-prevention within Australian prisons (SToP-C): a prospective cohort study. Lancet Gastroenterol Hepatol. 2021;6:533-46.[PubMed Abstract] -
- 64.Yang TH, Fang YJ, Hsu SJ, et al. Microelimination of Chronic Hepatitis C by Universal Screening Plus Direct-Acting Antivirals for Incarcerated Persons in Taiwan. Open Forum Infect Dis. 2020;7:ofaa301.[PubMed Abstract] -
- 65.Doyle JS, van Santen DK, Iser D, et al. Microelimination of Hepatitis C Among People With Human Immunodeficiency Virus Coinfection: Declining Incidence and Prevalence Accompanying a Multicenter Treatment Scale-up Trial. Clin Infect Dis. 2021;73:e2164-e2172.[PubMed Abstract] -
- 66.Olafsson S, Fridriksdottir RH, Love TJ, et al. Cascade of care during the first 36 months of the treatment as prevention for hepatitis C (TraP HepC) programme in Iceland: a population-based study. Lancet Gastroenterol Hepatol. 2021;6:628-37.[PubMed Abstract] -
- 67.Chhatwal J, He T, Hur C, Lopez-Olivo MA. Direct-Acting Antiviral Agents for Patients With Hepatitis C Virus Genotype 1 Infection Are Cost-Saving. Clin Gastroenterol Hepatol. 2017;15:827-837.e8.[PubMed Abstract] -
- 68.Goel A, Chen Q, Chhatwal J, Aggarwal R. Cost-effectiveness of generic pan-genotypic sofosbuvir/velpatasvir versus genotype-dependent direct-acting antivirals for hepatitis C treatment. J Gastroenterol Hepatol. 2018;33:2029-36.[PubMed Abstract] -
- 69.He T, Lopez-Olivo MA, Hur C, Chhatwal J. Systematic review: cost-effectiveness of direct-acting antivirals for treatment of hepatitis C genotypes 2-6. Aliment Pharmacol Ther. 2017;46:711-721.[PubMed Abstract] -
- 70.Padula WV, Levin JS, Lee J, Anderson GF. Cost-effectiveness of total state coverage for hepatitis C medications. Am J Manag Care. 2021;27:e171-e177.[PubMed Abstract] -
- 71.Roebuck MC. Impact of direct-acting antiviral use for chronic hepatitis C on health care costs in Medicaid: economic model update. Am J Manag Care. 2022;28:630-1.[PubMed Abstract] -
Additional References
- AASLD-IDSA. HCV Guidance: Recommendations for testing, management, and treating hepatitis C. Retreatment of persons in whom prior therapy failed.
- Asselah T, Bourgeois S, Pianko S, et al. Sofosbuvir/velpatasvir in patients with hepatitis C virus genotypes 1-6 and compensated cirrhosis or advanced fibrosis. Liver Int. 2018;38:443-450.[PubMed Abstract] -
- Benhammou JN, Dong TS, May FP, et al. Race affects SVR12 in a large and ethnically diverse hepatitis C-infected patient population following treatment with direct-acting antivirals: Analysis of a single-center Department of Veterans Affairs cohort. Pharmacol Res Perspect. 2018;6:e00379.[PubMed Abstract] -
- Cabibbo G, Petta S, Calvaruso V, et al. Is early recurrence of hepatocellular carcinoma in HCV cirrhotic patients affected by treatment with direct-acting antivirals? A prospective multicentre study. Aliment Pharmacol Ther. 2017;46:688-95.[PubMed Abstract] -
- El-Sherif O, Jiang ZG, Tapper EB, et al. Baseline Factors Associated With Improvements in Decompensated Cirrhosis After Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection. Gastroenterology. 2018;154:2111-2121.e8.[PubMed Abstract] -
- Falade-Nwulia O, Suarez-Cuervo C, Nelson DR, Fried MW, Segal JB, Sulkowski MS. Oral Direct-Acting Agent Therapy for Hepatitis C Virus Infection: A Systematic Review. Ann Intern Med. 2017;166:637-48.[PubMed Abstract] -
- Fernández-Montero JV, Aspinall EJ, Burns JE. Treatment as Prevention: Should Hepatitis C Learn the Lessons from HIV? AIDS Rev. 2017;19:212-218.[PubMed Abstract] -
- Martin NK, Hickman M, Hutchinson SJ, Goldberg DJ, Vickerman P. Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy. Clin Infect Dis. 2013;57 Suppl 2:S39-45.[PubMed Abstract] -
- Olafsson S, Tyrfingsson T, Runarsdottir V, et al. Treatment as Prevention for Hepatitis C (TraP Hep C) - a nationwide elimination programme in Iceland using direct-acting antiviral agents. J Intern Med. 2018;283:500-7.[PubMed Abstract] -
- Pol S, Parlati L. Treatment of hepatitis C: the use of the new pangenotypic direct-acting antivirals in "special populations". Liver Int. 2018;38 Suppl 1:28-33.[PubMed Abstract] -
- Reig M, Mariño Z, Perelló C, et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J Hepatol. 2016;65:719-726.[PubMed Abstract] -
- Waziry R, Hajarizadeh B, Grebely J, et al. Hepatocellular carcinoma risk following direct-acting antiviral HCV therapy: A systematic review, meta-analyses, and meta-regression. J Hepatol. 2017;67:1204-1212.[PubMed Abstract] -
- Zeuzem S, Foster GR, Wang S, et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection. N Engl J Med. 2018;378:354-369.[PubMed Abstract] -
- Zuckerman A, Chastain CA, Naggie S. Retreatment Options Following HCV Direct Acting Antiviral Failure. Curr Treat Options Infect Dis. 2017;9:389-402.[PubMed Abstract] -
Figures
 Figure 1 (Image Series). Sustained Virologic Response 12 (SVR 12)This graphic shows an example of an SVR12 in a person who received 8 weeks of HCV DAA therapy. The SVR12 is shown by the undetectable HCV RNA 12 weeks after treatment was stopped.Source: illustration by David H. Spach, MD
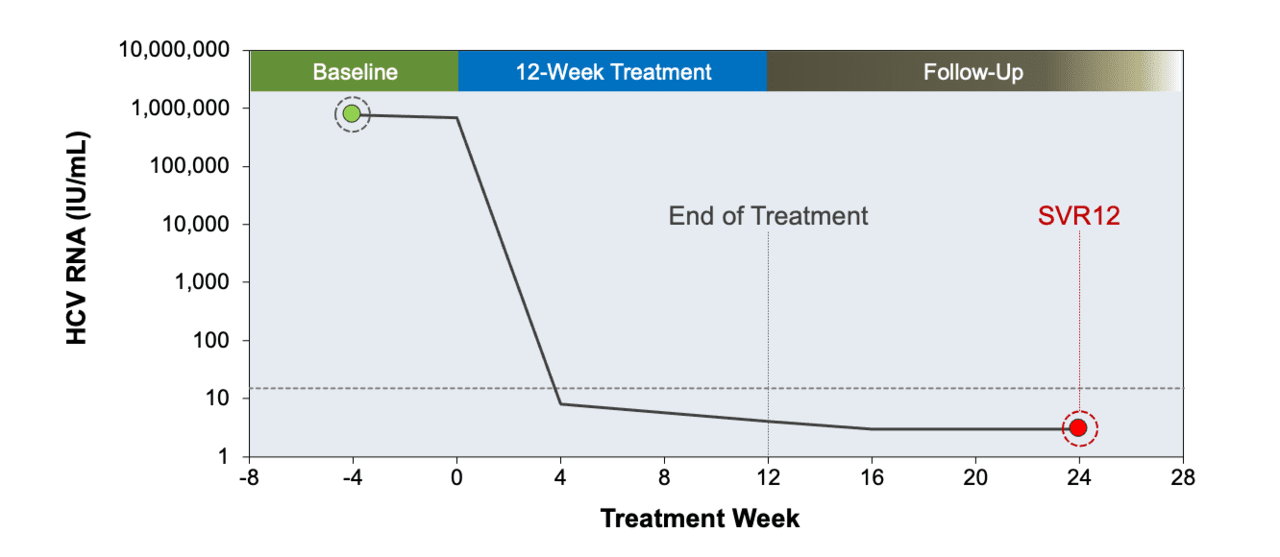
Figure 1 (Image Series). Sustained Virologic Response 12 (SVR 12)This graphic shows an example of an SVR12 in a person who received 8 weeks of HCV DAA therapy. The SVR12 is shown by the undetectable HCV RNA 12 weeks after treatment was stopped.Source: illustration by David H. Spach, MD Figure 1B. SVR 12 After 12-Week HCV Treatment CourseThis graphic shows an example of an SVR12 in a person who received 12 weeks of HCV DAA therapy. The SVR12 is shown by the undetectable HCV RNA 12 weeks after treatment was stopped.Source: illustration by David H. Spach, MD
Figure 1B. SVR 12 After 12-Week HCV Treatment CourseThis graphic shows an example of an SVR12 in a person who received 12 weeks of HCV DAA therapy. The SVR12 is shown by the undetectable HCV RNA 12 weeks after treatment was stopped.Source: illustration by David H. Spach, MD Figure 2. Liver Stiffness in Persons With or Without SVR12This graph compares liver stiffness before and after treatment in adults who attained SVR12 versus those who did not achieve SVR12.Source: Singh S, Facciorusso A, Loomba R, Falck-Ytter YT. Magnitude and Kinetics of Decrease in Liver Stiffness After Antiviral Therapy in Patients With Chronic Hepatitis C: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16:27-38.e4.
Figure 2. Liver Stiffness in Persons With or Without SVR12This graph compares liver stiffness before and after treatment in adults who attained SVR12 versus those who did not achieve SVR12.Source: Singh S, Facciorusso A, Loomba R, Falck-Ytter YT. Magnitude and Kinetics of Decrease in Liver Stiffness After Antiviral Therapy in Patients With Chronic Hepatitis C: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16:27-38.e4. Figure 3. Median Liver Stiffness Treatments in Persons Treated with Direct-Acting Antiviral TherapySource: Chan J, Gogela N, Zheng H, et al. Direct-Acting Antiviral Therapy for Chronic HCV Infection Results in Liver Stiffness Regression Over 12 Months Post-treatment. Dig Dis Sci. 2018;63:486-92.
Figure 3. Median Liver Stiffness Treatments in Persons Treated with Direct-Acting Antiviral TherapySource: Chan J, Gogela N, Zheng H, et al. Direct-Acting Antiviral Therapy for Chronic HCV Infection Results in Liver Stiffness Regression Over 12 Months Post-treatment. Dig Dis Sci. 2018;63:486-92. Figure 4. HCV Treatment and Outcome of Extrahepatic ManifestationsSource: Mahale P, Engels EA, Li R, et al. The effect of sustained virological response on the risk of extrahepatic manifestations of hepatitis C virus infection. Gut. 2018;67:553-61.
Figure 4. HCV Treatment and Outcome of Extrahepatic ManifestationsSource: Mahale P, Engels EA, Li R, et al. The effect of sustained virological response on the risk of extrahepatic manifestations of hepatitis C virus infection. Gut. 2018;67:553-61. Figure 5. Clinical Outcome by Response to Treatment in Patients with Chronic Hepatitis C and Advanced FibrosisSource: Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med. 2007;147:677-84.
Figure 5. Clinical Outcome by Response to Treatment in Patients with Chronic Hepatitis C and Advanced FibrosisSource: Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med. 2007;147:677-84. Figure 6. 5-Year Mortality Rate following HCV Treatment Based on SVR ResponseThis graphic is based on data from 31 studies published from 2000 to 2014 that included 33,360 participants. The 5-year mortality rates shown are based on whether the patient achieved an SVR.Source: Simmons B, Saleem J, Heath K, Cooke GS, Hill A. Long-Term Treatment Outcomes of Patients Infected With Hepatitis C Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response. Clin Infect Dis. 2015;61:730-40.
Figure 6. 5-Year Mortality Rate following HCV Treatment Based on SVR ResponseThis graphic is based on data from 31 studies published from 2000 to 2014 that included 33,360 participants. The 5-year mortality rates shown are based on whether the patient achieved an SVR.Source: Simmons B, Saleem J, Heath K, Cooke GS, Hill A. Long-Term Treatment Outcomes of Patients Infected With Hepatitis C Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response. Clin Infect Dis. 2015;61:730-40. Figure 7. Impact of SVR on Mortality Rates with DAA TherapySource: Backus LI, Belperio PS, Shahoumian TA, Mole LA. Direct-Acting Antiviral Sustained Virologic Response: Impact on Mortality in Patients without Advanced Liver Disease. Hepatology. 2018 Jan 29. [Epub ahead of print]
Figure 7. Impact of SVR on Mortality Rates with DAA TherapySource: Backus LI, Belperio PS, Shahoumian TA, Mole LA. Direct-Acting Antiviral Sustained Virologic Response: Impact on Mortality in Patients without Advanced Liver Disease. Hepatology. 2018 Jan 29. [Epub ahead of print]
Centers for Disease Control and Prevention (CDC)
Cooperative Agreement (CDC-RFA-PS21-2105)



Since you've received 80% or better on this quiz, you may claim continuing education credit.
You seem to have a popup blocker enabled. If you want to skip this dialog please Always allow popup windows for the online course.