Pathogenesis of Portal Hypertension
In persons with cirrhosis, portal hypertension is characterized by an increase in intrahepatic vascular resistance and increased portal blood flow.[1,2,3] The increased resistance in the liver results from architectural distortion due to fibrosis and regenerative nodules combined with increased intrahepatic vasoconstriction due to decreased endogenous nitric oxide production and endothelial dysfunction. In the presence of angiogenic factors and increased nitrous oxide production in the splanchnic vascular bed, splanchnic arteriolar vasodilatation and increased cardiac output increase portal venous blood inflow.[3,4]
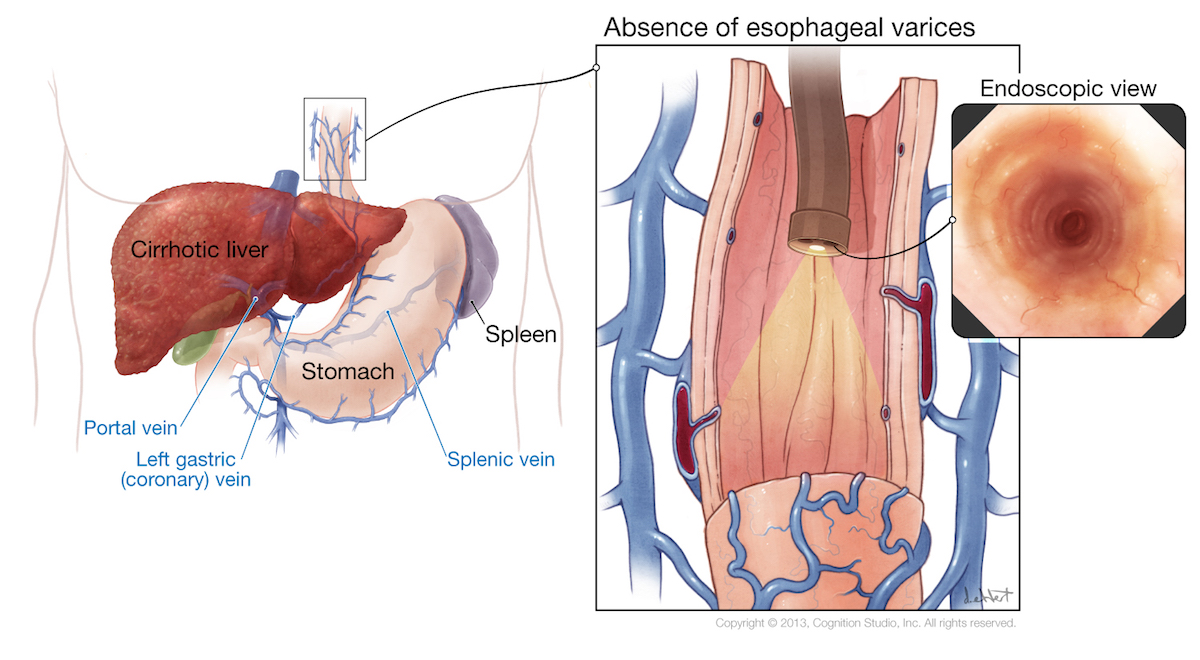
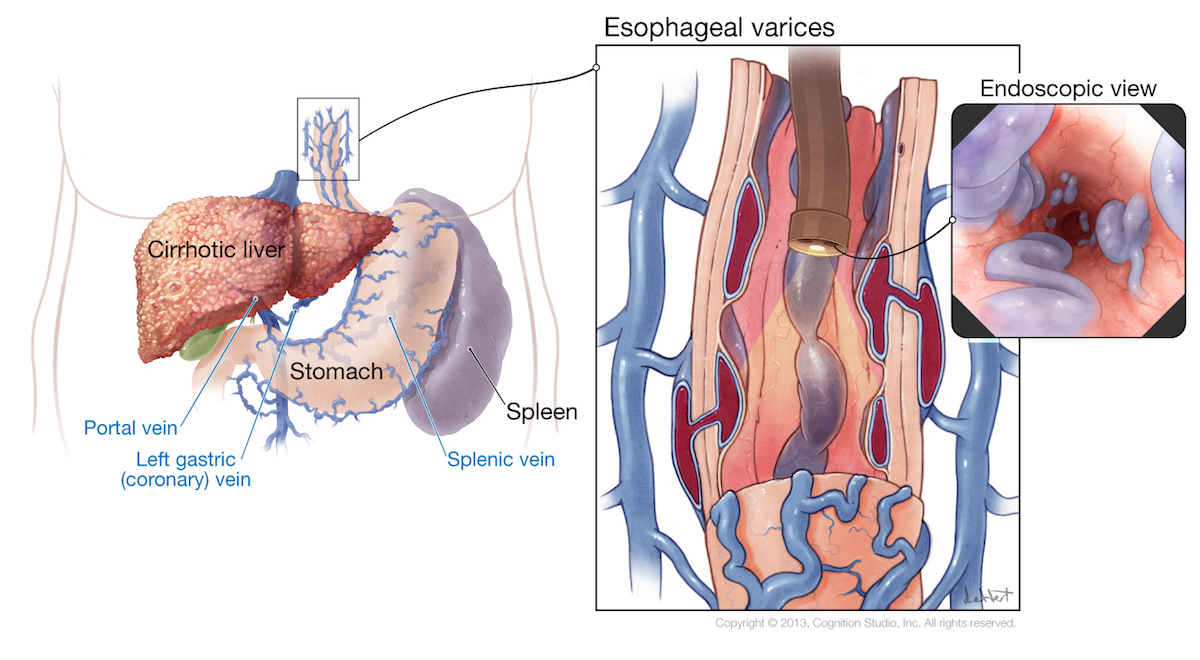
Portosystemic Collaterals
Collaterals develop in response to the portal hypertension at sites of communication between the portal and systemic circulations; these collaterals are accompanied by splanchnic vasodilatation.[2,3] In comparison to other collaterals, gastroesophageal varices are important due to their risk of rupture and bleeding.
Hepatic Venous Pressure Gradient
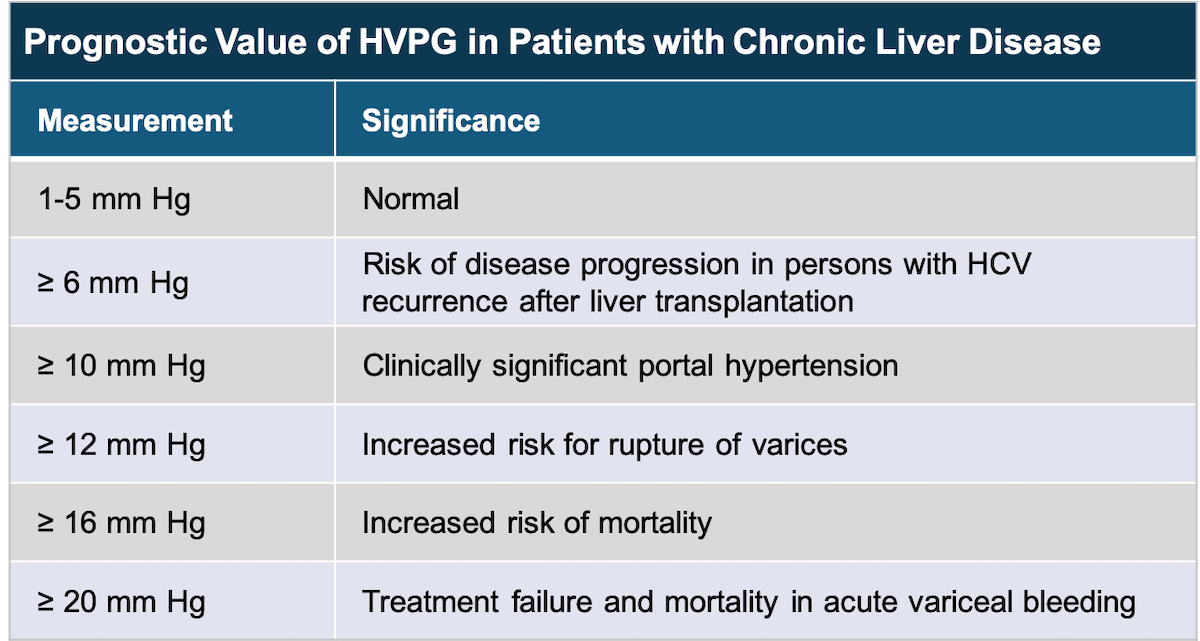
The hepatic venous pressure gradient is a measure of portal (sinusoidal) pressure and can be obtained by passing a balloon catheter under radiologic guidance into the hepatic vein via the jugular or femoral vein.[3,4] The free hepatic vein pressure is subtracted from the wedged hepatic vein pressure to calculate the hepatic venous pressure gradient, which normally is 3 to 5 mm Hg, and an elevated value indicates an intrahepatic cause of portal hypertension.[3,4] Due to the invasive nature of the procedure used to obtain the hepatic venous pressure gradient, it is not widely used in the United States for prognostic or therapeutic monitoring purposes.[3,5] The hepatic venous pressure gradient predicts the risk of developing varices and overall prognosis (Figure 1).[3,5] It can also be followed to monitor response to therapy and progression of liver disease. The following definitions summarize contemporary definitions for portal hypertension based on the hepatic venous pressure gradient.[1,2,4]
- Portal Hypertension: any hepatic venous pressure gradient greater than 5 mm Hg is considered as portal hypertension.
- Mild Portal Hypertension: defined as a hepatic venous pressure gradient greater than 5 mm Hg but less than 10 mm Hg.
- Clinically Significant Portal Hypertension: defined as hepatic venous pressure gradient value of 10 mm Hg or greater.