 Elbasvir-Grazoprevir Zepatier
Elbasvir-Grazoprevir Zepatier Glecaprevir-Pibrentasvir Mavyret
Glecaprevir-Pibrentasvir Mavyret Ledipasvir-Sofosbuvir Harvoni
Ledipasvir-Sofosbuvir Harvoni Ribavirin Copegus, Rebetol, Ribasphere
Ribavirin Copegus, Rebetol, Ribasphere Sofosbuvir Sovaldi
Sofosbuvir Sovaldi Sofosbuvir-Velpatasvir Epclusa
Sofosbuvir-Velpatasvir Epclusa Sofosbuvir-Velpatasvir-Voxilaprevir Vosevi
Sofosbuvir-Velpatasvir-Voxilaprevir VoseviMultiple studies have shown that successful antiviral therapy of chronic hepatitis C virus (HCV) infection dramatically reduces both liver-related morbidity (including rates of end-stage liver disease and hepatocellular carcinoma) and mortality, as well as all-cause mortality.[1,2,3,4] Direct-acting antiviral (DAA) treatment for HCV has proven to be much safer, better tolerated, and more effective than treatments used in the interferon era, now rendering the decision to initiate therapy much easier. Cure rates with HCV treatment using modern pangenotypic DAA regimens are greater than 95%.[5,6,7] The AASLD-IDSA HCV Guidance notes that evidence clearly supports treatment of nearly all persons with chronic HCV infection.[8] Decisions regarding initiating therapy will naturally be influenced by the individual’s willingness and readiness to undertake treatment.
Evaluation and Preparation for Hepatitis C Treatment
Making a Decision on When to Initiate HCV Therapy
- Module 4 Overview
Evaluation and Preparation for Hepatitis C Treatment - Lesson 1
Goals and Benefits with HCV TreatmentActivitiesLesson 2. Making a Decision on When to Initiate HCV Therapy
Learning Objective Performance Indicators
- Summarize current recommendations for HCV treatment indications in persons with chronic HCV
- List absolute contradictions for HCV treatment with direct-acting antiviral therapy
- Discuss relative contradictions for HCV treatment with direct-acting antiviral therapy
- Describe key patient readiness factors to assess prior to initiating treatment
- Outline general monitoring recommendations when HCV treatment is deferred
Last Updated: April 1st, 2024Author:Maria A. Corcorran, MD, MPHMaria A. Corcorran, MD, MPH
Assistant Professor
Division of Allergy & Infectious Diseases
University of WashingtonReviewer:David H. Spach, MDDavid H. Spach, MD
Professor of Medicine
Division of Allergy & Infectious Diseases
University of WashingtonDisclosures: NoneTable of ContentsBackground
Indications for HCV Treatment
The AASLD-IDSA HCV Guidance previously provided a priority ranking for treatment based on clinical factors and public health considerations.[8] This priority ranking arose, in part, due to the relatively limited infrastructure capable of treating the surge of persons with chronic HCV infection who had been waiting to receive treatment with new DAA therapy.[8] This treatment priority ranking is no longer used in the AASLD-IDSA HCV Guidance and is no longer considered clinically appropriate. Instead, the current guidance emphasizes that all persons should receive treatment for chronic HCV infection, except those individuals with a short (i.e., less than 12 months) life expectancy that cannot be modified by HCV treatment, liver transplantation, or another therapy.[8] The recommendation to treat virtually all persons with chronic HCV infection stems from multiple factors, including the very high sustained virologic response (SVR) rates with current DAA therapy, the safety and tolerability of DAA therapy, and the preponderance of data demonstrating benefit across a spectrum of clinical outcomes with achievement of SVR.[8,9]
Contraindications for Treatment
Absolute Contraindications
In the DAA era, there are relatively few absolute contraindications to HCV treatment with DAAs. The AASLD-IDSA HCV Guidance recommends against treating persons with a short life expectancy that cannot be improved by HCV treatment, liver transplantation, or another directed therapy.[8] Available data from animal studies indicate that ribavirin has significant teratogenic and embryocidal adverse effects.[10] Accordingly, the use of ribavirin is contraindicated in women who are pregnant, women who may become pregnant, or men whose female partners are pregnant or trying to conceive.[11,12] Persons with chronic HCV who are of reproductive age and are to receive a regimen that includes ribavirin should be advised to use at least two forms of contraception during treatment and for at least 6 months following the end of treatment.[13] With DAA therapy, decompensated cirrhosis, renal failure, and recent or active substance use (e.g., drugs and alcohol) are not contraindications to treatment.[14,15,16] Indeed, multiple studies involving persons with past or current injection drug use have shown very good adherence and excellent SVR rates with HCV DAA therapy.[17,18,19,20]
Relative Contraindications
In addition to some absolute contraindications, there are several situations in which the clinician should exert careful consideration before starting HCV treatment, including chaotic social circumstances and decompensated mental health disorders that may significantly impact an individual’s ability to adhere to therapy.[21,22] Since there are no large-scale studies on the use of pangenotypic DAA regimens during pregnancy, the AASLD-IDSA HCV Guidance recommends initiation of HCV therapy before trying to conceive.[8] There are, however, phase 1 and observational trial data from a few very small studies that suggest DAAs are likely safe during pregnancy, and as such, the AASLD-IDSA HCV Guidance states that treatment during pregnancy can be considered on an individual basis after engaging in shared decision-making.[8] For children with HCV, DAA therapy should be deferred until at least 3 years of age, as there are no approved DAA regimens for children younger than 3 years of age.[8]
Treatment Readiness
Assessing Readiness
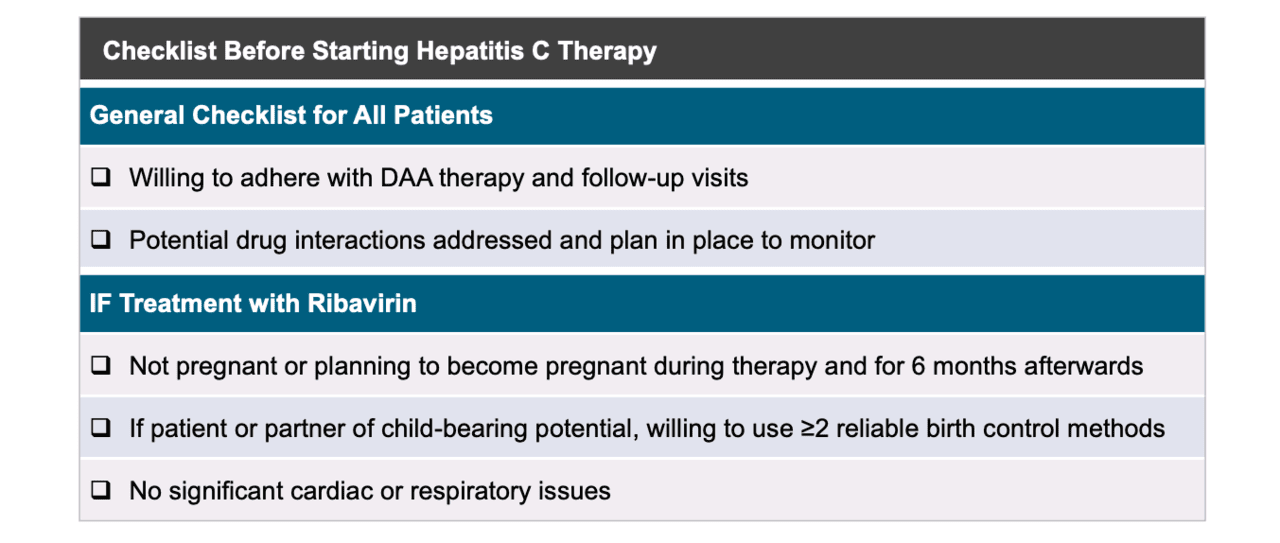
An individual’s readiness to start therapy can be difficult to assess, but a checklist can be used as a general guide (Figure 1). It is important to have a frank discussion with each person considering HCV treatment about the chance of cure, the potential side effects of therapy, the cost of treatment, and, if using a regimen that includes ribavirin, the impact of treatment on their quality of life, including deferring pregnancy.
Pretreatment Counseling
In addition, the HCV pretreatment discussion should cover counseling, drug interactions, potential side effects, specific information on follow-up visits, and the importance of good adherence.
Timing of Initiation of Treatment
The availability of DAAs has provided tremendous opportunities for highly effective, convenient, well-tolerated therapy. Although the high cost of these medications remains a concern, the cost of DAA therapy has significantly decreased over the past several years, and many states are now covering DAA therapy for all Medicaid and Medicare patients without restriction. The Center for Health Law and Policy Innovation of Harvard Law School (CHLPI) and the National Viral Hepatitis Roundtable (NVHR) has created a website that provides up-to-date information on state-by-state requirements for prior authorization for HCV treatment (2024 National Snapshot Report). Nevertheless, some state Medicaid plans continue to have fibrosis, sobriety, and medical prescriber restrictions for DAA therapy.[23] These restrictions are not in step with AASLD-IDSA HCV Guidance and represent a suboptimal and short-sighted approach to care.[8,24,25,26] If possible, DAA therapy should be initiated in all persons with chronic HCV and not deferred due to ongoing substance use or fibrosis requirements.
Advanced Age and Comorbid Conditions
Many persons living with chronic HCV in the United States are older than 50 years of age. With the availability of new, highly effective, safe, well-tolerated regimens, it is likely that more interest and experience will accumulate in treating persons of advanced age. Notably, some clinical trials with newer direct-acting antivirals have enrolled persons older than 70 years of age, but overall, relatively little experience exists with treatment of HCV in elderly populations. Despite this, there is no contraindication for treating patients of an older age, although careful attention should be paid to the potential for drug interactions, which may be more common in elderly individuals on multiple medications. For older individuals with HCV who have limited life expectancy due to other comorbid conditions, HCV treatment is unlikely to alter their quality of life or life expectancy, and thus, in some situations involving persons with advanced age or significant medical comorbidities associated with an expected short lifespan (less than 12 months), it may be sensible to withhold therapy.
Obtaining Authorization and Payment for Medications
Due to the cost of DAAs, prior authorization may be needed for some medical plans. The authorization process may take weeks, with the exact time dependent on the insurance coverage and state of residence. Restrictions vary by state and insurer as to who can prescribe DAAs, as well as the level of fibrosis and sobriety. In states where restrictions exist, individuals with HCV waiting to start treatment should be warned in advance that the DAA medication approval process may be drawn out.
Monitoring and Follow-Up if Not Treated
General Recommendations for Monitoring and Follow-Up
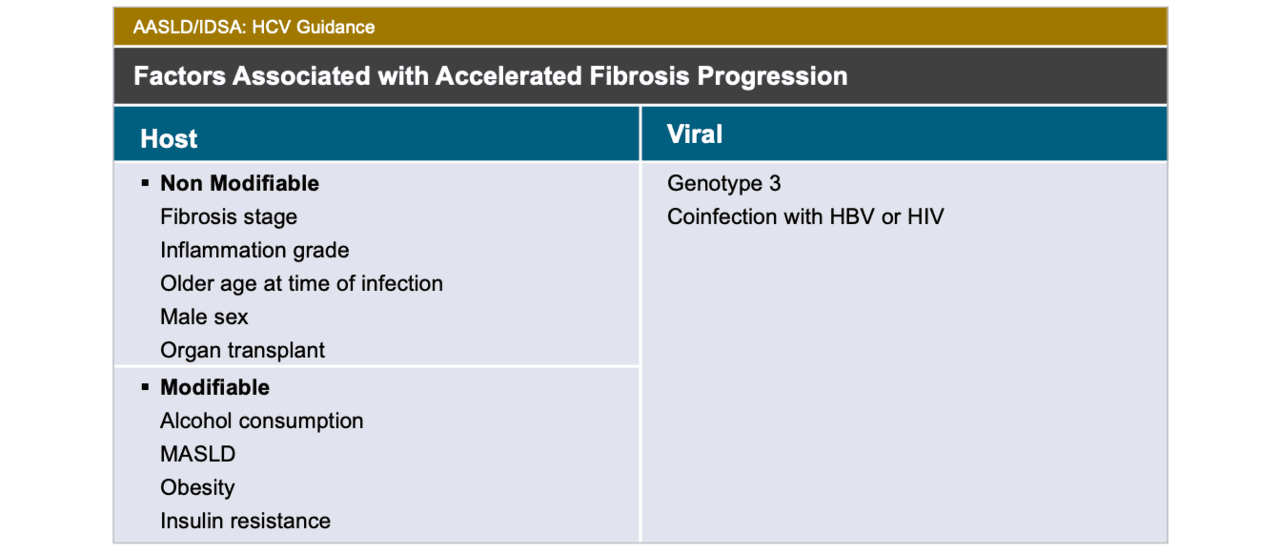
There may be various reasons for deferring HCV treatment, including specific barriers that are present for the individual considering treatment, such as active psychosocial instability, competing medical priorities, or other temporary barriers. At least annual follow-up is recommended for these individuals. During these follow-up visits, counseling should occur regarding behaviors that will optimize liver health, including avoiding a diet high in saturated fat, achieving a healthy body weight, limiting intake of hepatotoxic medications, and abstaining from or limiting alcohol intake. Medical providers should be aware of indicators associated with accelerated hepatic fibrosis progression, such as older age at the time of HCV infection, male sex, alcohol consumption, metabolic dysfunction-associated steatotic liver disease (MASLD), metabolic-dysfunction associated steatohepatitis (MASH), HCV genotype 3, and coinfection with HIV and/or hepatitis B virus (HBV) (Figure 2).[27,28,29] Individuals who have indicators associated with accelerated hepatic fibrosis should receive counseling regarding the risk and impact of accelerated hepatic fibrosis progression; in this setting, clinicians should attempt to promptly initiate HCV treatment. These individuals also should receive information and education on the warning signs and symptoms of liver dysfunction, including jaundice, melena, clay-colored stools, confusion, abdominal distention, and lower extremity edema.[30,31] Finally, persons with chronic HCV should receive counseling on HCV transmission and strategies on how to prevent transmission of HCV to others.
Reassessing Hepatic Fibrosis
Among individuals with chronic HCV and mild to moderate fibrosis (F0 to F2), progression of liver fibrosis can occur. As such, they should undergo annual monitoring with laboratory studies that include aspartate aminotransferase (AST), alanine aminotransferase (ALT), complete blood cell count (CBC), and platelet count. From these basic laboratory tests, an AST to Platelet Ratio Index (APRI) and/or a FIB-4 index can be calculated.[32,33] In addition, subsequent noninvasive testing to reevaluate hepatic fibrosis, such as FibroSure, FibroTest, ActiTest, or transient elastography, is recommended.[34,35] The optimal interval for reevaluating hepatic fibrosis may depend on clinical factors and the stage of liver disease. For individuals with cirrhosis, hepatocellular carcinoma (HCC) surveillance with a liver ultrasound and alpha-fetoprotein (AFP), is recommended approximately every 6 months.[36,37]
Monitoring and Assistance with an Unstable Psychosocial Situation
Although not a contraindication to treatment, individuals living with chronic HCV who have an unstable psychosocial situation should have these issues addressed by referring to appropriate resources, such as a mental health professional or a substance use disorder counselor. Ongoing alcohol use disorder is a high priority to address since it can markedly accelerate hepatic fibrosis; for this reason, persons with chronic HCV should receive a clear and strong counseling message to completely abstain from alcohol intake.[34,38] Special effort should be made to address psychosocial issues in persons with advanced fibrosis (F3 or F4), since they have a more immediate need for HCV treatment.
Summary Points
- The availability of highly effective, convenient, safe, well-tolerated therapy has changed the landscape for HCV treatment.
- Nearly all persons with chronic HCV will benefit from therapy; persons with a severely limited lifespan (less than 12 months) are the exception.
- The use of ribavirin is contraindicated in pregnancy; persons of reproductive age with chronic HCV who receive a regimen that includes ribavirin should be advised to use at least two forms of contraception during treatment and for at least 6 months following the end of treatment.
- For nearly all persons with chronic HCV, DAAs should be initiated and not be deferred due to ongoing substance use or fibrosis requirements of some state Medicaid plans and/or insurers.
- In situations when HCV treatment is deferred (for whatever reason), the individual should periodically undergo reevaluation for disease progression and reconsideration of treatment, with the frequency of reevaluation individualized based on the person’s current fibrosis stage, likely fibrosis progression rate, and other factors that may influence treatment readiness.
Citations
- 1.Veldt BJ, Heathcote EJ, Wedemeyer H, et al. Sustained virologic response and clinical outcomes in patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med. 2007;147:677-84.[PubMed Abstract] -
- 2.van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012 ;308:2584-93.[PubMed Abstract] -
- 3.Tada T, Kumada T, Toyoda H, et al. Viral eradication reduces all-cause mortality, including non-liver-related disease, in patients with progressive hepatitis C virus-related fibrosis. J Gastroenterol Hepatol. 2017;32:687-694.[PubMed Abstract] -
- 4.Morgan RL, Baack B, Smith BD, Yartel A, Pitasi M, Falck-Ytter Y. Eradication of hepatitis C virus infection and the development of hepatocellular carcinoma: a meta-analysis of observational studies. Ann Intern Med. 2013;158:329-37.[PubMed Abstract] -
- 5.Asselah T, Kowdley KV, Zadeikis N, et al. Efficacy of Glecaprevir/Pibrentasvir for 8 or 12 Weeks in Patients With Hepatitis C Virus Genotype 2, 4, 5, or 6 Infection Without Cirrhosis. Clin Gastroenterol Hepatol. 2018;16:417-26.[PubMed Abstract] -
- 6.Feld JJ, Jacobson IM, Hézode C, et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection. N Engl J Med. 2015;373:2599-607.[PubMed Abstract] -
- 7.Zeuzem S, Foster GR, Wang S, et al. Glecaprevir-Pibrentasvir for 8 or 12 Weeks in HCV Genotype 1 or 3 Infection. N Engl J Med. 2018;378:354-69.[PubMed Abstract] -
- 8.AASLD-IDSA. HCV Guidance: Recommendations for testing, management, and treating hepatitis C. When and in whom to initiate HCV therapy.
- 9.Marcellin F, Roux P, Protopopescu C, Duracinsky M, Spire B, Carrieri MP. Patient-reported outcomes with direct-acting antivirals for the treatment of chronic hepatitis C: current knowledge and outstanding issues. Expert Rev Gastroenterol Hepatol. 2017;11:259-268.[PubMed Abstract] -
- 10.Ferm VH, Willhite C, Kilham L. Teratogenic effects of ribavirin on hamster and rat embryos. Teratology. 1978;17:93-101.[PubMed Abstract] -
- 11.Feld JJ, Jacobson IM, Sulkowski MS, Poordad F, Tatsch F, Pawlotsky JM. Ribavirin revisited in the era of direct-acting antiviral therapy for hepatitis C virus infection. Liver Int. 2017;37:5-18.[PubMed Abstract] -
- 12.Roberts SS, Miller RK, Jones JK, et al. The Ribavirin Pregnancy Registry: Findings after 5 years of enrollment, 2003-2009. Birth Defects Res A Clin Mol Teratol. 2010;88:551-9.[PubMed Abstract] -
- 13.Ward RP, Kugelmas M. Using pegylated interferon and ribavirin to treat patients with chronic hepatitis C. Am Fam Physician. 2005;72:655-62.[PubMed Abstract] -
- 14.Charlton M, Everson GT, Flamm SL, et al. Ledipasvir and sofosbuvir plus ribavirin for treatment of HCV infection in patients with advanced liver disease. Gastroenterology. 2015;149:649-59.[PubMed Abstract] -
- 15.Cacoub P, Desbois AC, Isnard-Bagnis C, Rocatello D, Ferri C. Hepatitis C virus infection and chronic kidney disease: Time for reappraisal. J Hepatol. 2016;65:S82-S94.[PubMed Abstract] -
- 16.Gane E, Lawitz E, Pugatch D, et al. Glecaprevir and Pibrentasvir in Patients with HCV and Severe Renal Impairment. N Engl J Med. 2017;377:1448-55.[PubMed Abstract] -
- 17.Grebely J, Hajarizadeh B, Dore GJ. Direct-acting antiviral agents for HCV infection affecting people who inject drugs. Nat Rev Gastroenterol Hepatol. 2017;14:641-651.[PubMed Abstract] -
- 18.Grebely J, Dalgard O, Conway B, et al. Sofosbuvir and velpatasvir for hepatitis C virus infection in people with recent injection drug use (SIMPLIFY): an open-label, single-arm, phase 4, multicentre trial. Lancet Gastroenterol Hepatol. 2018;3:153-61.[PubMed Abstract] -
- 19.Beer L, Inglis S, Malaguti A, et al. Randomized clinical trial: Direct-acting antivirals as treatment for hepatitis C in people who inject drugs: Delivered in needle and syringe programs via directly observed therapy versus fortnightly collection. J Viral Hepat. 2022;29:646-53.[PubMed Abstract] -
- 20.Litwin AH, Lum PJ, Taylor LE, et al. Patient-centred models of hepatitis C treatment for people who inject drugs: a multicentre, pragmatic randomised trial. Lancet Gastroenterol Hepatol. 2022;7:1112-27.[PubMed Abstract] -
- 21.Grebely J, Oser M, Taylor LE, Dore GJ. Breaking down the barriers to hepatitis C virus (HCV) treatment among individuals with HCV/HIV coinfection: action required at the system, provider, and patient levels. J Infect Dis. 2013;207 Suppl 1:S19-25.[PubMed Abstract] -
- 22.Meyer JP, Moghimi Y, Marcus R, Lim JK, Litwin AH, Altice FL. Evidence-based interventions to enhance assessment, treatment, and adherence in the chronic Hepatitis C care continuum. Int J Drug Policy. 2015;26:922-35.[PubMed Abstract] -
- 23.Hepatitis C. State of Medicaid Access. Center for Health Law and Policy Innovation of Harvard Law School (CHLPI) and the National Viral Hepatitis Roundtable (NVHR).[CHLPI and NVHR] -
- 24.Zahnd C, Salazar-Vizcaya L, Dufour JF, et al. Modelling the impact of deferring HCV treatment on liver-related complications in HIV coinfected men who have sex with men. J Hepatol. 2016;65:26-32.[PubMed Abstract] -
- 25.Butt AA, Yan P. Natural history of hepatitis C virus infection in a large national seroconversion cohort in the direct-acting antiviral agent era: Results from ERCHIVES. J Viral Hepat. 2021 Mar 24. Online ahead of print.[PubMed Abstract] -
- 26.Sahakyan Y, Lee-Kim V, Bremner KE, Bielecki JM, Krahn MD. Impact of direct-acting antiviral regimens on mortality and morbidity outcomes in patients with chronic hepatitis c: Systematic review and meta-analysis. J Viral Hepat. 2021 Feb 8. Online ahead of print.[PubMed Abstract] -
- 27.Lingala S, Ghany MG. Natural History of Hepatitis C. Gastroenterol Clin North Am. 2015;44:717-34.[PubMed Abstract] -
- 28.Maasoumy B, Wedemeyer H. Natural history of acute and chronic hepatitis C. Best Pract Res Clin Gastroenterol. 2012;26:401-12.[PubMed Abstract] -
- 29.Poynard T, Morra R, Halfon P, et al. Meta-analyses of FibroTest diagnostic value in chronic liver disease. BMC Gastroenterol. 2007;7:40.[PubMed Abstract] -
- 30.Heidelbaugh JJ, Bruderly M. Cirrhosis and chronic liver failure: part I. Diagnosis and evaluation. Am Fam Physician.2006;74:756-62.[PubMed Abstract] -
- 31.Udell JA, Wang CS, Tinmouth J, et al. Does this patient with liver disease have cirrhosis? JAMA. 2012;307:832-42.
[PubMed Abstract] -
- 32.Wai CT, Greenson JK, Fontana RJ, Kalbfleisch JD, Marrero JA, Conjeevaram HS, Lok AS. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518-26.[PubMed Abstract] -
- 33.Lin ZH, Xin YN, Dong QJ, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatology. 2011;53:726-36.[PubMed Abstract] -
- 34.Poynard T, Ratziu V, Charlotte F, Goodman Z, McHutchison J, Albrecht J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. J Hepatol. 2001;34:730-9.[PubMed Abstract] -
- 35.Afdhal NH. Fibroscan (transient elastography) for the measurement of liver fibrosis. Gastroenterol Hepatol (N Y). 2012;8:605-7.[PubMed Abstract] -
- 36.Singal AG, Llovet JM, Yarchoan M, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78:1922-65.[AASLD] -
- 37.AASLD-IDSA. HCV Guidance: Recommendations for testing, management, and treating hepatitis C. Monitoring patients who are starting HCV treatment, are on treatment, or have completed therapy.
- 38.Wiley TE, McCarthy M, Breidi L, McCarthy M, Layden TJ. Impact of alcohol on the histological and clinical progression of hepatitis C infection. Hepatology. 1998;28:805-9.[PubMed Abstract] -
Additional References
- Chappell CA, Scarsi KK, Kirby BJ, et al. Ledipasvir plus sofosbuvir in pregnant women with hepatitis C virus infection: a phase 1 pharmacokinetic study. Lancet Microbe. 2020;1:e200-e208.[PubMed Abstract] -
- Dore GJ, Altice F, Litwin AH, et al. Elbasvir-Grazoprevir to Treat Hepatitis C Virus Infection in Persons Receiving Opioid Agonist Therapy: A Randomized Trial. Ann Intern Med. 2016;165:625-634.[PubMed Abstract] -
- Graham CS, Baden LR, Yu E, Mrus JM, Carnie J, Heeren T, Koziel MJ. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta-analysis. Clin Infect Dis. 2001;33:562-9.[PubMed Abstract] -
- Grebely J, Dore GJ, Zeuzem S, et al. Efficacy and Safety of Sofosbuvir/Velpatasvir in Patients With Chronic Hepatitis C Virus Infection Receiving Opioid Substitution Therapy: Analysis of Phase 3 ASTRAL Trials. Clin Infect Dis. 2016;63:1479-1481.[PubMed Abstract] -
- Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358-80.[PubMed Abstract] -
- Hellard ME, Jenkinson R, Higgs P, et al. Modelling antiviral treatment to prevent hepatitis C infection among people who inject drugs in Victoria, Australia. Med J Aust. 2012;196:638-41.[PubMed Abstract] -
- Martin NK, Hickman M, Hutchinson SJ, Goldberg DJ, Vickerman P. Combination interventions to prevent HCV transmission among people who inject drugs: modeling the impact of antiviral treatment, needle and syringe programs, and opiate substitution therapy. Clin Infect Dis. 2013;57 Suppl 2:S39-45.[PubMed Abstract] -
- Martin NK, Vickerman P, Grebely J, et al. Hepatitis C virus treatment for prevention among people who inject drugs: Modeling treatment scale-up in the age of direct-acting antivirals. Hepatology. 2013;58:1598-609.[PubMed Abstract] -
- Missiha SB, Ostrowski M, Heathcote EJ. Disease progression in chronic hepatitis C: modifiable and nonmodifiable factors. Gastroenterology. 2008;134;1699-714.[PubMed Abstract] -
- Poynard T, Bedossa P, Opolon P. Lancet. Natural history of liver fibrosis progression in patients with chronic hepatitis C. The OBSVIRC, METAVIR, CLINIVIR, and DOSVIRC groups. Lancet. 1997;349:825-32.[PubMed Abstract] -
- Schmid P, Bregenzer A, Huber M, et al. Progression of Liver Fibrosis in HIV/HCV Co-Infection: A Comparison between Non-Invasive Assessment Methods and Liver Biopsy. PLoS One. 2015;10:e0138838.[PubMed Abstract] -
- Thomas DL, Villano SA, Riester KA, et al. Perinatal transmission of hepatitis C virus from human immunodeficiency virus type 1-infected mothers. Women and Infants Transmission Study. J Infect Dis. 1998;177:1480-8.[PubMed Abstract] -
- Yattoo GN, Shafi SM, Dar GA, et al. Safety and efficacy of treatment for chronic hepatitis C during pregnancy: A prospective observational study in Srinagar, India. Clin Liver Dis (Hoboken). 2023;22:134-9.[PubMed Abstract] -
Figures
 Figure 1. Suggested Checklist Prior to Initiating Treatment for Chronic HCVAbbreviations: DAA = direct-acting antiviral
Figure 1. Suggested Checklist Prior to Initiating Treatment for Chronic HCVAbbreviations: DAA = direct-acting antiviral Figure 2. Factors Associated with Accelerated Hepatic FibrosisAbbreviations: MASLD = metabolic dysfunction-associated steatotic liver diseaseSource: American Association for the Study of Liver Disease, the Infectious Diseases Society of America. When and in whom to initiate HCV therapy. Recommendations for testing, management, and treating hepatitis C.
Figure 2. Factors Associated with Accelerated Hepatic FibrosisAbbreviations: MASLD = metabolic dysfunction-associated steatotic liver diseaseSource: American Association for the Study of Liver Disease, the Infectious Diseases Society of America. When and in whom to initiate HCV therapy. Recommendations for testing, management, and treating hepatitis C.
Since you've received 80% or better on this quiz, you may claim continuing education credit.
You seem to have a popup blocker enabled. If you want to skip this dialog please Always allow popup windows for the online course.